Seladelpar as a PPAR-δ Agonist in Pbc: Pharmacological Insights and Clinical Applications
 and Gayatri S *
and Gayatri S *Sri Ramachandra Faculty of Pharmacy, SRIHER (DU), Chennai. Tamil Nadu, India.
Corresponding Author E-mail:gayatrisru@yahoo.co.in
DOI : http://dx.doi.org/10.13005/ojc/420108
Download this article as:
![]()
Primary biliary cholangitis (PBC) is an autoimmune disease that is characterized by the continuous destruction of small bile ducts within the liver, primarily affecting women aged 40-65. The condition leads to cholestasis and potential liver failure, necessitating effective treatment strategies. Seladelpar (MBX-8025) is a novel selective peroxisome proliferator-activated receptor (PPAR)-delta agonist that has been pioneered to address the unmet need in PBC management. Recent trials demonstrate that seladelpar significantly reduces alkaline phosphatase (ALP) levels and improves patients overall biochemical response, particularly in those intolerant or nonresponsive to UDCA. Particularly, seladelpar regulates bile acid metabolism via suppression of CYP7A1 and elevation of FGF21, contributing to its anti-inflammatory and antifibrotic actions. As a promising experimental drug, seladelpar could reshape treatment approach for PBC, providing an alternative treatment for patients who do not respond adequately to existing therapies due to inadequate responses.
KEYWORDS:Bile acid metabolism; Biopharmaceutical innovation; Liver fibrosis; Primary biliary cholangitis; PPAR-δ agonist; Seladelpar
Introduction
Primary biliary cholangitis (PBC) is a chronic autoimmune liver disease which results in the destruction of small bile ducts. 1 Approximately 1 in 1,000 middle-aged women more than 40 years have been extensively diagnosed with PBC, primarily involving the women aged 40-65 years. The pathogenesis is due to a combination of genetic susceptibility, environmental stimuli, and immune dysregulation. In addition to this, antimitochondrial antibodies (AMAs) occur in approximately 90-95% of PBC patients, which is a valuable diagnostic marker.2 The immune system destroys small intrahepatic bile ducts in this complex condition, thereby resulting in cholestasis, or the blockage of bile flow. The accumulation of cytotoxic bile acids due to this obstruction play a vital role for chronic inflammation and fibrosis, leading to biliary cirrhosis and eventually liver failure. The chronic, immune-mediated cytotoxicity for biliary epithelial cells produces progressive ductopenia and ultimately results in liver fibrosis.3,4
Increased amounts of total bilirubin and alkaline phosphatase (ALP) are the two independent risk factors in patients with PBC.5 The ideal approach is to normalize these bilirubin and ALP levels.6 OCA, a bile acid analog and farnesoid X receptor (FXR) agonist, is the only alternative approved for PBC.7,8 However, OCA treatment may provoke or intensify pruritus in a dose-proportional manner.9
In recent years, PPAR agonists have garnered interest as prospective treatments for PBC and other cholestatic disorders.10 PPARδ is activated by fatty acids and is essential for lipid metabolism and inflammatory conditions. Genes found in the Parenchymal cell of the liver, Kupffer’s cells, and Perisinusoidal cells within the liver are controlled by PPARδ. PPARδ is essential for regulating the homeostasis of bile acids, and it possesses antifibrotic characteristics.11,12 Seladelpar is a new, powerful, and selective first-in-class PPAR-δ agonist under development for treating PBC in individuals who are nonresponsive to or intolerant of UDCA.13,14
Methodology of Literature Review
This review was conducted to thoroughly assess the therapeutic potential, pharmacological properties, and clinical evidence supporting Seladelpar’s use in treating Primary Biliary Cholangitis (PBC). The methodology followed a structured, narrative review approach, focusing on identifying and synthesizing peer-reviewed literature and clinical trial data. A comprehensive literature search was performed in the following electronic databases: PubMed, Science Direct, Google Scholar, ClinicalTrials.gov, and EMBASE. The search used various combinations of the following keywords and Medical Subject Headings (MeSH) terms: “Seladelpar,” “Primary biliary cholangitis,” “PPAR-delta agonist,” “Cholestatic liver disease,” “Liver fibrosis,” “Bile acid metabolism,” and “Clinical Trial Seladelpar.” Search results were limited to articles published in English between 2015 and 2025.
Article Selection and Data Extraction
Titles and abstracts were screened for relevance, and full-text articles were retrieved for all potentially eligible studies.
Data were gathered using a standardized form that included:
Study design
Population characteristics
Intervention details (Seladelpar dosage and duration)
Outcome measures (e.g., ALP levels, pruritus improvement)
Adverse events and safety profile
Individual study findings were summarized qualitatively, emphasizing Seladelpar’s:
Mechanism of action
Clinical efficacy
Pharmacokinetic and pharmacodynamic properties
Safety and tolerability
Potential therapeutic applications beyond PBC
Comparisons were made with existing PBC treatments, especially UDCA and OCA, to contextualize Seladelpar’s role in the treatment landscape.
Mechanism of Action of Seladelpar
In preclinical models, seladelpar not only suppressed inflammatory cytokines but also had a role in modulating hepatic stellate cells that play a central role in fibrogenesis. The drug’s effect on energy metabolism is supported by its action on mitochondrial ß-oxidation and lipid utilization. These actions lead to decreased hepatic steatosis and liver histological improvement, particularly in cholestatic and metabolic liver disease models15-17
PPARs are nuclear hormone receptors with three members – PPAR-alpha (α), PPAR-delta (δ), and PPAR-gamma (γ).15 All three PPARs play roles in the regulation of energy homeostasis and metabolic function, including bile acid synthesis, fatty acid metabolism, and adipocyte differentiation.16 Both chronic liver conditions, such as PBC and NASH, feature changes in the bile acid composition and elevated systemic bile acids.
Despite being a PPAR-delta agonist, seladelpar’s mode of action in treating PBC patients is still poorly known. One pharmacological action that may have a bearing on treatment outcomes is the suppression of bile acid production via PPARδ activation.14 Published literature shows that activation of PPARδ by seladelpar reduces synthesis of bile acids by promoting FGF21, leading to the activation of JNK signaling pathway: this process leads to the repression of CYP7A1-the main enzyme responsible for synthesizing bile acids from cholesterol. The farnesoid X receptor pathway is the molecular mechanism that controls bile acid production in the liver. This pathway is not involved in the inhibition of bile acid synthesis by seladelpar.14,16
Seladelpar inhibited the synthesis of bile acids in the hepatocytes via decreasing the plasma C4 marker, which is directly linked with BA synthesis, while simultaneously it inhibited the vital enzyme, CYP7A1, in that pathway, and decreased its building blocks, cholesterol for synthesis, thus leading to an even stronger anti-cholestatic action. According to P. Boudes et al., it inhibits stellate cells, causing liver fibrosis, Kupffer cells and infiltrating macrophages within the liver. Clinically, the subsequent anti-inflammatory effect is shown by decreasing high-sensitivity C-reactive protein and transaminases.17
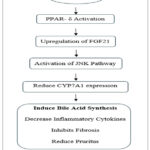 |
Figure 1: Mechanism of Seladelpar. Click here to View table |
Clinical Trial Data
Several clinical trials have been carried out to assess the efficacy and safety of Seladelpar in patients with primary biliary cholangitis (PBC). Table 1 summarizes key findings from major Phase 2 and Phase 3 trials.
Table 1: Summary of Seladelpar Clinical Trials
| Trial Name | Phase | Design | Population | Key Findings | Adverse Events | References |
| Phase 2 Study | Phase 2 | Randomized, Open-label; 52-week study | PBC patients with inadequate UDCA response | Dose-dependent reduction in ALP,
Biochemical response maintained over 52 weeks, Reduce pruritus
|
Well tolerated, minimal withdrawals | [18] |
| RESPONSE | Phase 3 | Double-blinded, Placebo-controlled | UDCA non-responders | 61.7 % achieved composite endpoint, Significant reduction in ALP, Reduced pruritus | Mild (headache, nausea, pruritus) | [19] |
| ENHANCE | Phase 3 | Double-blinded, Placebo-Controlled | UDCA-intolerant or non-responsive patients | Trial halted (external reason), Seladelpar ˃ Placebo in achieving biochemical targets | Mild pruritus, epigastric discomfort | [20] |
| ASSURE | Phase 3 | Open-label | PBC with compensated chirrhosis | Significant reduction in liver enzymes, Maintained efficacy with optimized dose | No major safety issues | [21] |
Currently, an open-label study (NCT04950764) is investigating the safety and tolerability of a 10 mg daily oral dose of seladelpar in PBC patients with hepatic impairment.22
Comparative Studies and Strategic Benefits
In the RESPONSE and ENHANCE studies, seladelpar consistently demonstrated superior results compared to placebo groups across multiple biochemical parameters, including ALP reduction, bilirubin normalization, and composite response.19,20 In the RESPONSE trial, 61.7% of patients treated with seladelpar achieved a composite response, versus 20% of those on placebo. Notably, 25% of seladelpar patients reached complete ALP normalization, while none in the placebo group did, which is especially significant given ALP’s role as a key predictor of long-term outcomes in PBC.5
Seladelpar’s favorable pharmacokinetic profile also improves its clinical usability. With a short half-life (about 6 hours) and minimal variability between individuals, once-daily dosing is both effective and convenient14 Additionally, the lack of a food effect on absorption offers flexibility in administration timing, potentially increasing adherence, particularly among elderly patients or those with complex medication schedules.
Pharmacokinetics
The pharmacokinetic profile of Seladelpar shows favorable features for clinical application. The main parameters related to its absorption, distribution, metabolism, and excretion are listed in Table 2.
Table 2: Pharmacokinetics of Seladelpar
| Parameters | Value |
| Absorption | Rapid, Dose-proportional exposure |
| Bioavailability | High |
| Half-life | 4-7 hours |
| Volume of Distribution (Vd) | 133.2 L |
| Oral Clearance (CL) | 12 L/hr |
| Food Effect | Minimal |
| Plasma Protein Binding | ˃99% |
| Excretion | 73.4 % excreted via urine & 19.5 % via faeces |
Metabolism
Seladelpar undergoes hepatic metabolism primarily via cytochrome P450 enzymes. The major metabolites, involved enzymes, and their pharmacokinetic characteristics are listed in Table 3.
Table 3: Seladelpar Metabolism and Metabolites
| Metabolite | CYP Enzymes Involved | AUC Ratio (Relative to Parent) | Median Tmax |
| Seladelpar Sulfoxide | CYP2C9 (major), CYP2C8, CYP3A4 | 0.36 | 10 hours |
| Desethyl-seladelpar | CYP2C9 (major), CYP2C8, CYP3A4 | 2.32 | 4 hours |
| Desethyl-seladelpar Sulfoxide | CYP2C9 (major), CYP2C8, CYP3A4 | 0.63 | 4 hours |
Pharmocodynamics
Seladelpar exerts its therapeutic effects in PBC by modulating bile acid metabolism. Fig 2 outlines its mechanism of action and the resulting clinical outcomes.14,15,18
 |
Figure 2: Pharmacodynamics of Seladelpar Click here to View Figure |
Source: U.S. Food and Drug Administration. LIVDELZI (seladelpar) prescribing information, 2024. Accessed May 30, 2025. FDA.gov and Kouno et al., J Biol Chem, 2022;298(7):102094.
Pharmacoecomic Impact
From a health economics perspective, seladelpar’s dual benefits—biochemical normalization and reduction in pruritus—along with its additional effects on fatigue and sleep, lead to tangible improvements in patient quality of life (QoL) and may reduce healthcare resource use. Quantifiable quality-of-life assessments like SF-36 and CLDQ have consistently shown improvement in patients taking seladelpar, with the most significant gains seen in mental health, vitality, and body pain domains [24]. When these benefits are projected over a patient’s lifetime, they can alleviate the burden on healthcare systems by decreasing hospitalizations and delaying the need for liver transplants.
Therapeutic Potential Beyond PBC
Although Seladelpar’s initial focus has been on treating PBC, its mechanism of action suggests it could also be effective for other metabolic and cholestatic liver conditions such as nonalcoholic steatohepatitis (NASH), primary sclerosing cholangitis (PSC), and autoimmune hepatitis. The drug’s ability to enhance mitochondrial function, decrease inflammatory cytokines, and alter lipid metabolism has already demonstrated effectiveness in NASH animal models.15
Additionally, its role in modulating FGF21 and inhibiting CYP7A1 offers a metabolic advantage, especially in bile acid imbalance disorders and hepatic steatosis. Initial research suggests that seladelpar can enhance insulin sensitivity and reduce hepatic lipid accumulation, making it a promising candidate for combination therapy in metabolic liver diseases.15,17
Drug Interactions
The exposure to seladelpar may increase when used with OAT3 inhibitors, CYP2C9 inhibitors, CYP3A4 inhibitors, or BCRP inhibitors. The systemic exposure of seladelpar may decrease when co-administered with bile acid sequestrants and rifampin.14
Adverse Drug Reactions
In clinical trials, some patients experienced mild transaminase elevations, which resolved either spontaneously or with dose adjustment. The drug’s safety monitoring protocols focus on regular liver function tests to detect any early signs of hepatotoxicity. Importantly, no deaths or life-threatening adverse reactions were directly linked to seladelpar in any trial cohort.14,19 Headache, nausea, stomach distension, dizziness, and abdominal discomfort are common adverse effects. Serious side effects include bone fractures, changes in liver tests, and worsening hepatic conditions such as ascites, jaundice of the skin or sclera, altered mental status, right upper quadrant abdominal pain, dysarthria, psychosis, melena or hematochezia, and blood expectoration.23
Warning and Precautions
Fractures occurred in 4% of patients treated with seladelpar.
Immediately stop seladelpar if a patient exhibits symptoms of hepatitis, such as jaundice, eosinophilia, or elevated liver enzymes (ALT, AST, TB, and/or alkaline phosphatase [ALP]). If hepatotoxicity occurs again after reintroducing seladelpar, consider permanently discontinuing the medication.
If biliary obstruction is suspected, discontinue seladelpar and treat as clinically indicated.14
Symptomatic Improvements
Pruritus
This included a subanalysis of secondary outcomes of symptoms related to an open-label, phase 2 trial of seladelpar. Earlier, 71% of patients experienced pruritus, and 29% of patients suffered from moderate to severe itching. By the end of an year of therapy, pruritus had improved markedly in 58% of the 5 or 10 mg group and in 93% of the 10 mg group.
Fatigue
Kremer et al. discovered that 10 mg of seladelpar improved the PBC-40 fatigue domain. Sixty-four percent of the 47 patients whose data were available had improved, twenty-one percent had become worse, and fifteen percent had not changed significantly. There were less notable changes in the 5 mg or 10 mg group: 38% worsened, 7% remained the same, and 55% improved.
Sleep disturbance
In the seladelpar early-stage clinical trial, more than half of the patients experienced sleep disturbances of varying intensity; however, sleep issues were assessed through general symptom questionnaires rather than tools specifically designed to measure sleep quality. 81% of the 5/10 mg cohort had no worsening of sleep disturbance on treatment, and 78% of the 10 mg cohort had a mean sleep score improvement, with improvement of pruritus being correlated with a notable amelioration of sleep disruption.
Beyond pruritus, fatigue, and disturbed sleep, patients also indicated improvement in their general quality of life by standardized HRQoL measurements in the form of the SF-36 and CLDQ questionnaires. Such improvements are matched with decreases in biochemical markers and affirm the complete value of seladelpar treatment in PBC.24
Ongoing Research and Safety Monitoring
Ongoing clinical trials, including NCT04950764, aim to further clarify the safety and efficacy of seladelpar in patients with liver disease. These trials are also highly relevant as they help determine dosing strategies for patients with varying liver function, from compensated cirrhosis. [22] Safety remains a top priority. While seladelpar has shown a largely favorable safety profile, with most adverse effects being mild to moderate, vigilant pharmacovigilance is still necessary. Four percent of patients developed fractures, raising concerns about long-term effects on bone mineral density, especially among postmenopausal women, a group primarily affected. [20] Further detailed analysis, including long-term registry data and bone density scans, is necessary to clarify these findings.
Regulatory Outlook and Accessibility
In February 2024, findings from landmark trials such as RESPONSE generated growing expectations of approval by regulators in key markets like the U.S., the E.U., and the Asia-Pacific nations [15]. However, as with most innovative therapies, access and cost remain significant challenges. Health policymakers need to work with pharmaceutical developers to ensure fair access, especially for underserved groups.
Limitations
Despite its promising profile, some limitations and questions remain. Firstly, long-term cardiovascular endpoints, malignancy risk, and effects in patients with advanced decompensated cirrhosis are still unknown. Secondly, the whole molecular interaction of PPARδ activation within the larger hepatic immune context remains to be clarified. Research into whether and how seladelpar interacts with other nuclear receptors, cytokine networks, and microbiota-mediated bile acid metabolism may uncover additional therapeutic options3,4,15
Future Directions
Seladelpar represents a significant advancement in PBC therapy, especially given the limitations of existing treatments like UDCA and OCA. UDCA remains the primary front-line treatment for PBC; however, nearly 40% of patients do not achieve satisfactory biochemical responses and require additional or alternative therapies.6-8 Although the FDA has approved OCA as a second-line option, its use is often limited by dose-related pruritus, which can adversely impact quality of life in PBC patients.9 In contrast, seladelpar not only does not worsen pruritus but also appears to significantly reduce it, as consistently shown in Phase 2 and Phase 3 trials [18,19,20]. Additionally, unlike FXR agonists such as OCA, seladelpar acts through the PPARδ pathway rather than the farnesoid X receptor, targeting the FGF21-JNK-CYP7A1 pathway. Its distinct mechanism allows it to effectively inhibit bile acid production without increasing systemic toxicity or pruritus.14,15 Furthermore, seladelpar has demonstrated anti-inflammatory and antifibrotic effects, suggesting benefits beyond biochemical improvement. Preclinical studies have shown its impact on hepatic stellate cells and Kupffer cells, indicating potential broader advantages in managing liver fibrosis.17
Conclusion
Thus, this novel PPAR-δ agonist has shown a promising results in clinical trials, demonstrating substantial reductions in ALP levels and improvements in overall biochemical responses. As ongoing studies continue to explore the full potential of seladelpar, its role in redefining treatment paradigms for PBC becomes increasingly apparent. Overall, the promising clinical outcomes associated with seladelpar offer hope for improved management of this challenging autoimmune disease, paving the way for better patient outcomes and the quality of life. In summary, Seladelpar’s introduction into clinical practice could mark a transformative step in the treatment of PBC, highlighting the importance of continued research and innovation in addressing unmet medical needs.
Acknowledgement
The authors thank Sri Ramachandra Faculty of Pharmacy, SRIHER (DU), Chennai, for their support in this review.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The author(s) do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
References
- Wetten, A., Jones, D.E.J. and Dyson, J.K. Seladelpar: an investigational drug for the treatment of early-stage primary biliary cholangitis (PBC). Expert Opinion on Investigational Drugs. 2022, 31(10), 1101-1107.
CrossRef - Webb, G.J., Siminovitch, K.A. and Hirschfield, G.M. The immunogenetics of primary biliary cirrhosis: a comprehensive review. Journal of autoimmunity. 2015, 64, 42-52.
CrossRef - Lleo, A., Wang, G.Q., Gershwin, M.E. and Hirschfield, G.M., 2020. Primary biliary cholangitis. The Lancet. 2020, 396(10266), 1915-1926.
CrossRef - Jansen, P.L., Ghallab, A., Vartak, N., Reif, R., Schaap, F.G., Hampe, J. and Hengstler, J.G. The ascending pathophysiology of cholestatic liver disease. Hepatology. 2017, 65(2), 722-738.
CrossRef - Panzitt, K. and Wagner, M. FXR in liver physiology: Multiple faces to regulate liver metabolism. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease. 2021; 1867(7), 166133.
CrossRef - Perez, C.F.M., Harms, M.H., Lindor, K.D., Van Buuren, H.R., Hirschfield, G.M., Corpechot, C., Van Der Meer, A.J., Feld, J.J., Gulamhusein, A., Lammers, W.J. and Ponsioen, C.Y. Goals of treatment for improved survival in primary biliary cholangitis: treatment target should be bilirubin within the normal range and normalization of alkaline phosphatase. Official journal of the American College of Gastroenterology| ACG. 2020, 115(7), 1066-1074.
CrossRef - Lindor, K.D., Bowlus, C.L., Boyer, J., Levy, C. and Mayo, M. Primary biliary cholangitis: 2018 practice guidance from the American Association for the Study of Liver Diseases. Hepatology. 2019, 69(1), 394-419.
CrossRef - Molinaro, A. and Marschall, H.U. Bile acid metabolism and FXR-mediated effects in human cholestatic liver disorders. Biochemical Society Transactions. 2022; 50(1), 361-373.
CrossRef - Nevens, F., Andreone, P., Mazzella, G., Strasser, S.I., Bowlus, C., Invernizzi, P., Drenth, J.P., Pockros, P.J., Regula, J., Beuers, U. and Trauner, M. A placebo-controlled trial of obeticholic acid in primary biliary cholangitis. New England Journal of Medicine. 2016, 375(7), 631-643.
CrossRef - Corpechot, C., Poupon, R. and Chazouillères, O. New treatments/targets for primary biliary cholangitis. JHEP Reports. 2019, 1(3), 203-213.
CrossRef - Li, Y., Wang, L., Yi, Q., Luo, L. and Xiong, Y. Regulation of bile acids and their receptor FXR in metabolic diseases. Frontiers in Nutrition. 2024; 11, 1447878.
CrossRef - Stofan, M. and Guo, G.L. Bile acids and FXR: novel targets for liver diseases. Frontiers in medicine. 2020; 7, 544.
CrossRef - Jones, D., Boudes, P. F., Swain, M. G., Bowlus, C. L., Galambos, M. R., Bacon, B. R., Doerffel, Y., Gitlin, N., Gordon, S. C., Odin, J. A., Sheridan, D., Wörns, M. A., Clark, V., Corless, L., Hartmann, H., Jonas, M. E., Kremer, A. E., Mells, G. F., Buggisch, P., Freilich, B. L., … Hirschfield, G. M. Seladelpar (MBX-8025), a selective PPAR-δ agonist, in patients with primary biliary cholangitis with an inadequate response to ursodeoxycholic acid: a double-blind, randomised, placebo-controlled, phase 2, proof-of-concept study. The lancet. Gastroenterology & hepatology. 2017,2(10), 716–726. https://doi.org/10.1016/S2468-1253(17)30246-7.
CrossRef - U.S. Food and Drug Administration. Approved Drug Products: LIVDELZI (seladelpar) capsules, for oral use. [Accessed May 30, 2025]. Available from: accessdata.fda.gov/drugsatfda_docs/label/2024/217899s000lbl.pdf
- Kouno, T., Liu, X., Zhao, H., Kisseleva, T., Cable, E. E., & Schnabl, B. (2022). Selective PPARδ agonist seladelpar suppresses bile acid synthesis by reducing hepatocyte CYP7A1 via the fibroblast growth factor 21 signaling pathway. The Journal of biological chemistry. 2022,298(7), 102056. https://doi.org/10.1016/j.jbc.2022.102056
CrossRef - Tian, S. Y., Chen, S. M., Pan, C. X., & Li, Y. FXR: structures, biology, and drug development for NASH and fibrosis diseases. Acta pharmacologica Sinica. 2022, 43(5), 1120–1132. https://doi.org/10.1038/s41401-021-00849-4.
CrossRef - Boudes, P., Choi, Y.J., Steinberg, A.S., Bergheanu, S. and Mcwherter, C. Seladelpar’s mechanism of action as a potential treatment for primary biliary cholangitis and non-alcoholic steato-hepatitis. Journal of Hepatology. 2018, 68, S235-S236.
CrossRef - Bowlus, C. L., Galambos, M. R., Aspinall, R. J., Hirschfield, G. M., Jones, D. E. J., Dörffel, Y., Gordon, S. C., Harrison, S. A., Kremer, A. E., Mayo, M. J., Thuluvath, P. J., Levy, C., Swain, M. G., Neff, G. W., Sheridan, D. A., Stanca, C. M., Berg, C. P., Goel, A., Shiffman, M. L., Vierling, J. M., … McWherter, C. A. A phase II, randomized, open-label, 52-week study of seladelpar in patients with primary biliary cholangitis. Journal of hepatology. 2022,77(2), 353–364. https://doi.org/10.1016/j.jhep.2022.02.033
CrossRef - Hirschfield, G. M., Shiffman, M. L., Gulamhusein, A., Kowdley, K. V., Vierling, J. M., Levy, C., Kremer, A. E., Zigmond, E., Andreone, P., Gordon, S. C., Bowlus, C. L., Lawitz, E. J., Aspinall, R. J., Pratt, D. S., Raikhelson, K., Gonzalez-Huezo, M. S., Heneghan, M. A., Jeong, S. H., Ladrón de Guevara, A. L., Mayo, M. J., … ENHANCE Study Group*. Seladelpar efficacy and safety at 3 months in patients with primary biliary cholangitis: ENHANCE, a phase 3, randomized, placebo-controlled study. Hepatology (Baltimore, Md.). 2023, 78(2), 397–415. https://doi.org/10.1097/HEP.0000000000000395.
CrossRef - Hirschfield, G. M., Bowlus, C. L., Mayo, M. J., Kremer, A. E., Vierling, J. M., Kowdley, K. V., Levy, C., Villamil, A., Ladrón de Guevara Cetina, A. L., Janczewska, E., Zigmond, E., Jeong, S. H., Yilmaz, Y., Kallis, Y., Corpechot, C., Buggisch, P., Invernizzi, P., Londoño Hurtado, M. C., Bergheanu, S., Yang, K., … RESPONSE Study Group (2024). A Phase 3 Trial of Seladelpar in Primary Biliary Cholangitis. The New England journal of medicine. 2024, 390(9), 783–794. https://doi.org/10.1056/NEJMoa2312100.
CrossRef - Gordon, S., Jacobson, I., Younes, Z., Silveira, M., Drenth, J., Morgera, U., Dalekos, G., Heo, J., Yang, K., Heusner, C. and Crittenden, D.B. Efficacy and Safety of Seladelpar in Patients With Primary Biliary Cholangitis and Compensated Liver Cirrhosis in the Open-Label, Long-Term ASSURE Safety Study: Interim Results. Zeitschrift für Gastroenterologie. 2025, 63(01),12-20.
CrossRef - ClinicalTrials.gov. Available from: Study Details | An Open-Label Study Following Oral Dosing of Seladelpar to Subjects With Primary Biliary Cholangitis (PBC) and Hepatic Impairment (HI) | ClinicalTrials.gov
- Drugs.com. Seladelpar. Available from: https://www.drugs.com/seladelpar.html
- Kremer, A. E., Mayo, M. J., Hirschfield, G., Levy, C., Bowlus, C. L., Jones, D. E., Steinberg, A., McWherter, C. A., & Choi, Y. J. Seladelpar improved measures of pruritus, sleep, and fatigue and decreased serum bile acids in patients with primary biliary cholangitis. Liver international : official journal of the International Association for the Study of the Liver. 2022, 42(1), 112–123. https://doi.org/10.1111/liv.15039
CrossRef
Accepted on: 10 Sep 2025







ISSN Online: 2231-5039

![]()




{kind=link}