Exploring the Pathophysiology, Epidemiology and Mechanisms of Asthma: Insights into Diagnosis, Prevention and Treatment in Pediatric Patients.
 , Tanzeel Ahmed1, Ankit Agrawal1and Basudev Banerjee2
, Tanzeel Ahmed1, Ankit Agrawal1and Basudev Banerjee21School of Biotechnology, IFTM University, Lodhipur Rajput, Delhi Road (NH-24), Moradabad, Uttar Pradesh, India.
2Department of Biochemistry, Santosh Deemed to be University, Santosh Nagar, Ghaziabad, Uttar Pradesh, India.
Corresponding Author E-mail: ankitbharduaj1990@gmail.com
DOI : http://dx.doi.org/10.13005/ojc/420202
Download this article as:
![]()
Asthma is one of the most common chronic respiratory disorders in children, characterized by airway inflammation, hyperresponsiveness, and reversible airflow obstruction. Its multifactorial pathophysiology involves complex interactions between genetic predisposition, immune dysregulation, and environmental triggers, leading to variable clinical manifestations. Epidemiological studies highlight the rising global prevalence of pediatric asthma, with substantial geographic and socioeconomic disparities that underscore the role of lifestyle, pollution, and early-life exposures in disease development. Asthma is a significant health concern in India, affecting about 35 million people out of a population of 1.36 billion. Asthma is a long lasting respiratory condition marked by air pathway inflammation, bronchoconstriction, and increased responsiveness. Asthma's pathophysiology involves complex inflammatory processes leading to airway remodeling, including fibrosis, smooth muscle hypertrophy, and mucus hypersecretion. Various transcription factors drive immune cell activation and cytokine production, promotes inflammation. Anti-inflammatory treatments, such as corticosteroids and leukotriene modifiers, aim to manage symptoms and prevent exacerbations. Genetic predispositions, particularly related to immune system regulation, and environmental exposures, significantly contribute to asthma's incidence. Immune markers like eosinophils, IgE, and fractional exhaled nitric oxide show promise in aiding diagnosis and monitoring disease progression. Preventive strategies, including allergen avoidance, smoking cessation, and vaccination, offer potential to reduce asthma risk and improve long-term outcomes. Understanding these multifaceted mechanisms is crucial for advancing both the diagnosis and management of asthma.
KEYWORDS:Asthma; Allergens; Corticosteroids; Eosinophils; Pollutants
Introduction
Bronchial asthma and its epidemiology
Asthma is a complex disease recognized by persistent air pathway inflammation and symptoms such as noisy breath, stiffness of chest, coughing, and shortness of breath. Asthma prevalence has increased significantly worldwide, in asthma most deaths occur in older adults and approximately 339 million people are affected by it (1). Severe asthma, affecting 1-29% of patients, accounts for over 60% of treatment costs.1 Asthma is the most common chronic disease in children, with varying prevalence across regions. Studies show 16% of the global adult population is clinically diagnosed with asthma, and 19.1% report symptoms.2 Low- and middle-income countries bear 84% of the global asthma burden and 96% of asthma-related deaths.3 In India the total burden of asthma estimated as 34.3 million which is accounting for 13.09% of the global burden given by Global Burden of Disease (GBD, 1990–2019).4 Even mild asthma can be fatal, with 30% of asthma-related deaths occurring in individuals with infrequent symptoms. Racial and socioeconomic disparities affect asthma diagnosis and treatment, with minorities facing higher morbidity and mortality rates. Misdiagnosis is common, with 12-50% of severe asthma diagnoses found to be inaccurate.
Mechanism associated with etiology of bronchial asthma
Inflammatory cells and Inflammation
Inflammation and asthma symptoms are not directly linked. Inflammation might inversely correlate with airway hyper responsiveness (AHR). Even when airways appear normal, due to mechanisms like mediator release from mast cells, abnormal smooth muscle activity, and airway wall thickening. Persistent inflammation heightens nerve sensitivity, leading to symptoms like coughing and chest tightness.5 Factors such as exercise can induce airway constriction in hyper responsive airways. Chronic inflammation and acute exacerbations define asthma, making it essential to understand these processes for effective management.6 Asthma etiology have precious role of immune cells and cytokines. Mast cells trigger acute bronchoconstrictor responses to allergens and stimuli like exercise and fog. Sensitized airway smooth muscle contains more mast cells. Prednisone treatment reduces tryptase-positive mast cells in asthma patients. Mast cells secrete interleukin (IL-4), sustaining allergic inflammation. Allergens activate mast cells via IgE. Low-affinity IgE receptors on macrophages in asthma patients allow allergen activation. Macrophages release cytokines, regulating inflammation, and can both initiate and resolve inflammation, affecting lymphocyte function after allergen exposure.7 Dendritic cells, have a crucial part in the pre stages of allergic reactions that can trigger asthma. They capture allergens, break them down into peptides, and carry them to nearby lymph nodes, where they initiate the formation of allergen-specific T lymphocytes. These immature dendritic cells facilitate the promotion of Th2 cell formation. Eosinophils infiltration is a hallmark of asthmatic airways.8 Eosinophils release basic proteins and free radicals, which contribute to airway hyperresponsiveness (AHR). They originate in the bone marrow and travel to the airways following allergen exposure. Their adhesion to vascular endothelial cells involves specific glycoprotein molecules (integrins) and adhesion compounds like ICAM-1, VLA4, and VCAM-1. The migration and existence of eosinophils in the air pathways are regulated by growth modulators like GM-CSF, IL-5cytokines and chemokines. Without growth stimuli, eosinophils undergo apoptosis. In mild to moderate chronic asthma Neutrophils are not the predominant cell type but they are more prominent in the induced sputum of individuals and airways and cause severe asthma. Drastic numbers of neutrophils are also investigated in the air pathway of asthma patients who die suddenly, potentially due to their quicker recruitment compared to eosinophils. T lymphocytes orchestrate the inflammatory action in asthma by releasing cytokines, which attract eosinophils and sustain mast cells. They produce cytokines like Dendritic cells, IL-13, IL-4 and IL-5, acting as antigen-presenting cells, program T lymphocytes. Children with atopy often maintain Th2 phenotype expression. A lack of childhood infections may promote Th2 cell formation, while early infections boost Th1 responses. Cytokines like IL-12, IL-4, and IL-13 regulate the Th1/Th2 balance, with IL-13 playing a major role in asthma. Structural cells, like fibroblasts and epithelial cells, generate inflammatory mediators and can be the primary source of persistent inflammation in asthma. Epithelial cells are key targets for inhaled glucocorticoids, translating environmental signals into an inflammatory response.9
Cytokines are pivotal in chronic inflammation and modulating the inflammatory response in asthma. They are produced by inflammatory cells (eosinophils, mast cells, lymphocytes, macrophages) and structural cells (endothelial and epithelial cells). Key cytokines essential for B-lymphocytes and VCAM-1 are IL-4 which produce IgE in endothelial cells for asthma. IL-3, necessary for mast cell survival in tissues. IL-4 and IL-5, crucial for eosinophil differentiation, existance, and priming. Spatially, IL-5 for eosinophil employment in asthma. Other cytokines like GM-CSF, IL-1b, IL-9, TNF-a and IL-6, also enhance the inflammatory response. TNF-a increases airway responsiveness and, along with IL-1b, activates post-inflammatory transcription regulators like AP-1 and NF-kB, leading to the activation of pro-inflammatory genes in the asthmatic airway.10 Anti-inflammatory cytokines like IL-1ra, IL-10, and PGE2 help reduce inflammation, but impaired IL-10 production in asthmatic patients may worsen symptoms. Other mediators, such as 15-HETE and lipoxins, also have anti-inflammatory effects. Adrenomedullin, produced in the lungs, may prevent macrophage cytokine release, but its role in asthma is not well understood. Macrophages and PGE2/IL-10 may help reduce inflammation, but macrophage-induced immunosuppression is diminished in asthma, promoting T cell proliferation.
Chronic inflammation in asthma leads to pathophysiological changes in airway cells, with ongoing inflammation and repair often seen as part of the disease.11 Despite advances in understanding, the connection between chronic inflammation and asthma symptoms remains unclear.11 The airway epithelium can be disrupted by various stimuli, such as viral infections, chemical sensitizers, and allergens.12 Asthmatics’ sputum or BAL fluid often contains clumps of epithelial cells, indicating poor adhesion. Epithelial injury may cause AHR through loss of barrier function, enzymes that break down inflammatory mediators, relaxant factors, or exposure of sensory nerves affecting airway reflexes.13 Asthma is marked by sudden inflammation causing airway obstruction, plasma leakage, dropsy, and phlegm. It is also a long lasting inflammatory disorder, with low-level allergens like mould and dust mites contributing to long-term airway changes, leading to gradual narrowing. These changes, which can explain the decline in airway function over time, include increased mucus-secreting cells, idiopathic pulmonary fibrosis, enlargement of smooth muscle, and vasculogenesis.14
Fibrosis and thickening of the smooth muscle lining the airway
In asthma, light microscopy shows a thicker basement membrane, but electron microscopy reveals that this is due idiopathic pulmonary fibrosis and the accumulation of type III and V collagen beneath the membrane.15 The thickness of this collagen is linked to chocking and responsiveness. Although the exact process for collagen accumulation is unclear, profibrotic mediators like endothelin-1, TGF-β, and PDGF released by macrophages or epithelial cells in inflamed airways are involved. Recent studies suggest mild mechanical stress can prompt airway epithelial cells to adopt a profibrotic phenotype.16 While sub epithelial fibrosis is found early in mild asthma, the role of collagen deposition and fibrosis in the disease remains uncertain.17
The role of smooth muscle abnormalities in asthmatic bronchial tubes remains debated. Asthmatic air pathway smooth muscle often doesn’t show heightened responses to spasmogens, potentially due to the ongoing inflammatory process.18 Long-term subjection to inflammatory cytokines, like IL-1b, can reduce the reaction to β2-adrenergic agonists, but steroid therapy may counteract this effect. Inflammatory mediators can alter β-adrenergic responses by affecting G protein signaling and ion channel activity, which influences smooth muscle excitability.19 Hypertrophy and hyperplasia of smooth muscle in asthmatics are likely caused by growth factors like PDGF and endothelin-1. Although inflammation causes vasodilatation, the impact of airway circulation in asthma is not fully understood, though studies show increased blood flow to the airway mucosa in asthmatics. This increased blood flow may influence airway diameter and contribute to conditions like exercise-induced asthma. Angiogenesis and microvascular leakage, driven by inflammatory mediators, may disrupt airway function by raising secretions, impairing mucociliary clearance, and promoting edema, leading to airway hyperresponsiveness.20
Neural effects
Recent research on brain processes in asthma has highlighted the role of nonadrenergic noncholinergic neurons and neuropeptides in airway control, alongside traditional cholinergic and adrenergic systems.21 Abnormalities in visceral function, such as heightened cholinergic and adrenergic responses or lower β-adrenergic responses, are thought to influence AHR, though these are considered secondary to the disease. Inflammation may link with self regulation by affecting neurotransmitter release through prejunctional receptors, as seen in histamine’s blockage of cholinergic neurotransmission and thromboxane’s facilitation of acetylcholine release.22 Inflammatory mediators can also sensitize sensory nerves, contributing to symptoms like cough and chest tightness. Neurotrophins may cause airway sensory nerves to become more sensitive. Asthma may result from a deficiency in nonadrenergic bronchodilator nerves, with VIP (vaso-active intestinal peptide) depletion observed in severe cases. Nitric oxide (NO) is also a key bronchodilator, and there may be a connection between VIP and NO. Inflammatory neuropeptides like substance P (SP) and neurokinin-A can prolong inflammation, with evidence of increased SP-immunoreactive nerves in severe asthma.23 This may result from nerve growth factor-induced sensory neuron proliferation and decreased neuropeptide degradation, contributing to persistent neurogenic inflammation
Redox imbalance
Free radicals, volatile atoms or molecules with unbonded electrons, are key mediators of cell damage and death. They include reactive oxygen species (e.g., superoxide anion, hyperoxide) and reactive nitrogen species (e.g., nitrous oxide, nitric oxides).24 These unstable molecules can inactivate enzymes, depolymerize polysaccharides, and damage DNA and cell membranes. Asthma, like other inflammatory diseases, is marked by increased oxidative stress due to reactive oxygen species produced by inflammatory cells. Asthmatic patients exhibit elevated levels of oxidative stress markers. Increased oxidative stress can exacerbate inflammation, decrease corticosteroid responsiveness, and correlate with asthma severity.25 Various markers for oxidative stress have examined biochemically. Lipid peroxidation interfere the form and purpose of cell and membrane of organelle, affecting their permeability, transport, and fluidity. Free radicals attacking membrane lipoproteins and polyunsaturated fatty acids produce malondialdehyde (MDA), which circulates in the bloodstream, causing further lipid peroxidation and cell death. MDA serves as a biomarker for oxidative stress, with its levels rising in acute asthma and correlating with asthma severity. A recent study highlighted an inverse relationship between nasal fluid MDA levels and asthma control in children, emphasizing MDA’s value as a biomarker for asthma management.26 Reduced glutathione (GSH) is a tripeptide consisting of -glutamyl-cysteinyl-glycine and is the most concentrated antioxidant in the airway epithelium lining fluid. In asthma, GSH detoxifies xenobiotics, scavenges free radicals, and regulates cellular functions like DNA synthesis and repair. Asthma symptoms worsen as GSH levels decrease. GSH levels in airway lavage fluid are higher than in the blood and further increases during asthma. Higher total glutathione levels in asthmatics correlate with lower levels of superoxide dismutase, ascorbate, and alpha-tocopherol. The rise in total glutathione is mainly due to increased glutathione disulfide (GSSG) levels. Glutathione-S-transferases (GST) facilitate detoxification by attaching GSH to reactive xenobiotic substrates and converting (H++e) to organic hydroperoxides, with glutathione peroxidases catalyzing the process.26 Nitric oxide (NO) is generated by various cells in the airways through NO synthases, but the precise biological source of NO in the lungs remains unidentified. Asthma patients exhibit elevated levels of exhaled NO, which probably reflect an inflammatory mechanism rather than a direct role in the pathogenesis of asthma. NO levels can be used to gauge local airway pH, impacting inflammation. Increased oxidative stress and NO can combine to form peroxynitrite, which nitrosylates proteins in the airways.27
Oxidative stress may also leads to various DNA lesions, such as strand breaks and nucleotide base modifications. Guanine is especially susceptible to oxidative changes, resulting in the formation of 8-hydroxydeoxyguanosine, a marker for DNA oxidation, which can cause mutations during replication. RNA, being closer to reactive species, is more frequently oxidized than DNA, leading to strand breaks and ribosomal malfunction, thus impacting protein synthesis. The homologous 8-hydroxyguanosine indicates RNA oxidation.28
Methodology involved in asthma incidence
Socio-economic status of environmental and prenatal tobacco smoking
Asthma vulnerability is linked to socioeconomic status, with children from lower socioeconomic backgrounds often experiencing higher asthma morbidity. Parental stress and family issues are also linked to higher asthma risk in children.29 Some studies show that children from low socioeconomic backgrounds in government schools are less likely to develop asthma, while factors like gender, smoke exposure, and household smoking contribute to higher asthma rates. Prenatal risk factors and varying wheezing conditions also complicate asthma assessments. Exposure to environmental tobacco smoke during pregnancy, particularly from smoking mothers, is strongly linked to wheezing symptoms and worsened asthma in children. It also increases the risk of developing severe asthma. Additionally, maternal smoking during pregnancy is linked to early childhood wheezing, reduced airway elasticity, and increased risks of food allergies, cytokine responses, and higher nitric oxide levels in infant exhaled air.29
Diet, nutrition through breastfeeding and stress
Epidemiological studies have focused on the effects of anti-inflammatory foods like polyunsaturated fatty acids and free radical scavengers like zinc and vitamin E on the development of atopic diseases.30 Up taking seafood or its oil during gestation is linked to a innocuous of eczema and atopic wheezing in children up to age 6.31 Higher maternity vitamin E and zinc levels are also associated with a reduced risk of wheezing up to age five.32 While caregiver stress is linked to higher immunoglobulin E levels and early wheeze in infants, no research has shown an association with asthma. Studies on prenatal antibiotic use have found a concentration effect relationship between the number of antibiotic application during pregnancy and the incidence of wheeze or asthma.33 The link between breastfeeding and asthma development is debated, with some studies suggesting protection and others showing exceeded rates of hypersensitivity and asthma in bottle-fed children.33 Exclusive breastfeeding for at least three months is associated with reduced asthma incidence, particularly in children with a family past of atopic reaction. However, some long-term studies indicate breastfeeding may boost the chances of atopic asthma, especially in children with an atopic mother.34 Diet restrictions during breastfeeding, such as excluding milk, eggs, and fish, have shown mixed results regarding the reduction of atopic dermatitis in infants. Prenatal and postnatal exposure to cigarette smoke has been linked to decreased airway caliber, which may contribute to wheezing and increased bronchial reactivity.35 Studies suggest that smaller airways in infancy may lead to persistent wheezing and asthma later in life, and children with recurrent wheezing show impaired lung function. Early lung impairment is often linked to maternal smoking and nicotine exposure, though other environmental factors have received less attention.36
Medication, Antibiotics, infections and allergic sensitization
Asthma may involve anti-inflammatory defects that increase airway inflammation. The diurnal drop in cortisol may contribute to nocturnal asthma worsening, with endogenous cortisol playing a key role in controlling allergic inflammation.37 Metyrapone, which reduces cortisol, can enhance allergic reactions. The enzyme 11b-hydroxysteroid dehydrogenase, which converts cortisol to cortisone, may function abnormally in asthma.38 Antibacterial application is linked to early croak and asthma, possibly through changes in intestinal flora, though higher wheezing rates don’t correlate with eczema or atopy.38 This suggests that other factors, such as viral infections in infancy, may play a role. Viral infections in early life can influence wheeze, and while they may lead to asthma in some children, they might be beneficial for others. Genetic predisposition and exposure to allergens or environmental factors, like air pollution and cigarette smoke, may also affect the risk of asthma. The relationship between infections, asthma, and allergy is still debated, with studies showing mixed results. Infections like respiratory syncytial virus or rhinovirus could contribute to chronic wheezing, though it remains unclear if infections alone cause asthma.39 An ancestory of asthma may increase the chances of recurrent respiratory infections in infants. Daycare attendance is linked to early wheezing but lower rates of chronic wheezing, possibly due to increased viral exposure. Asthma incidence is linked to blood immunoglobulin E (IgE) levels, a marker for allergen sensitivity, though high IgE levels at birth are associated more with atopy and aeroallergen sensitivity than with asthma. Asthma development, particularly in relation to allergens like cat, cockroach, and dust mites, is influenced by immune responses. A reduced interferon response at 3 months has been linked to increased chances of wheeze. Neonatal immune immaturity may favor Th2 responses, promoting atopy but not necessarily persistent asthma.40 Recent studies suggest variety in Toll-like receptors may play a key role in immune responses associated with asthma. Asthma can also stem from allergic rhinitis, with 10-40% of individuals with rhinitis also having asthma. Chronic rhino sinusitis, especially with polyps, is linked to more severe asthma.41
Genetic influences in asthma
Research on the genetics of asthma mainly focuses on atopy, which offers limited insight into asthma mechanisms.42 While genetics contribute to atopy, with multiple genes implicated, environmental factors like allergen exposure and infections play a larger role in whether atopic individuals develop asthma. However, genetics influence asthma severity and treatment response. Polymorphisms in genes involved in inflammation, such as cytokine production, may help predict asthma progression. Single-nucleotide polymorphisms (SNPs) could predict asthma outcomes, although this remains untested. Genotypic differences in pharmacological targets, like the b2-adrenoceptor and ALOX-5, influence treatment responses, highlighting genetics’ role in asthma management. Asthma development is influenced by various genes, which may differ across populations. Gene polymorphisms, such as those in FOXO3A, gasdermin-B, IL-4, IL-13, beta-2-adrenergic receptor, ADAM33, and STAT6, contribute to asthma severity.43 (43). For example, IL-10 gene haplotypes linked to increased production are associated with mild asthma, while those linked to lower building are linked with serious asthma. A variety in the IL-4 gene promoter is also linked to reduced lung function in severe asthma. Understanding the clustering of these genes is crucial for studying asthma susceptibility.44
Gene -environmental interactions and their relation to sex and gender
Asthma gene-environment interactions are complex. Some genes, like those encoding glutathione transferase, help detoxify inhaled substances, while other exposures influence expression of gene through non-inherited processes such as methylation DNA or histone manipulation.45 Phenotypic differences in monozygotic twins are thought to arise from epigenetic changes. Lifestyle choices and chemical exposures may affect disease risk through epigenetic alterations.45 Early life factors, including nutrition, smoking, microbial exposure, maternal stress, and care, may modify genetic expression and influence hypersensitivity and asthma development, though more research is required to confirm these effects. Asthma development is influenced by sex in a time-dependent manner.46 Boys have higher asthma incidence and severity up to age 6-12, with more hospitalizations.47 However, ladies experience more serious asthma, including more hospital requirements, longer stays, and higher readmission rates. These differences are thought to be linked to puberty. Males show greater airway hyperresponsiveness in childhood, while females experience it more severely in adulthood.48 Atopy is more common in boys before age 13, but by adulthood, its prevalence is similar in both sexes.49 Environmental factors like allergies affect males and females differently. Obesity has a stronger impact on asthma development in women, with some studies suggesting a causal relationship, though mechanisms remain unclear.
Occupational asthma
Asthma due to workplace exposures is common in various industries, including car painting (isocyanates), hairdressing (chemicals), cleaning (solutions), healthcare (latex), and baking (flour dust). A study of 6,837 individuals found that workplace chemical exposure increased the risk of new-onset asthma, particularly asthma with airway hyperresponsiveness. Nursing had the highest risk among occupations. Acute inhalation events, such as fires or chemical spills, further increased asthma risk. Occupational exposure contributed to 10-25% of adult asthma cases. Smoking marijuana or tobacco can cause asthma-like symptoms, and heart failure should be considered in the differential diagnosis of new-onset asthma.50 While atopy’s role as a risk factor decreases with age, it can still trigger asthma in adults. Air pollution generally worsens existing asthma rather than causing new cases. Asthma incidence and prevalence have increased over the past few decades, particularly in developed countries, but the underlying immunologic, genetic, and environmental mechanisms remain unclear.47 Some risk factors, like avoiding occupational sensitizers during pregnancy and early postpartum, are well-established. However, recent studies challenge earlier recommendations on avoiding animals and extended breastfeeding to reduce asthma risk. Discrepancies in exposures and outcomes may be clarified through gene-environment interaction and epigenetic research. While the rise in asthma cases may have plateaued in high-prevalence countries, primary prevention remains elusive, and reducing risk continues to be a key focus in asthma care.51
Diagnosis of bronchial asthma and immune markers
Asthma presents in various phenotypes, including allergic, non-allergic, late-onset, obesity-related, and persistent airflow limitation. Usual indications like noisy and reduced breath, coughing, and chest stiffness, often worsened at night and triggered by factors like influenza, physical exertion, allergens, or weather changes. A thorough asthma evaluation is required, considering prior episodes. Spirometry is used to assess lung function, with FEV1/FCV ratios below normal indicating asthma.52 A positive bronchodilator test shows an increase in FEV1 of >12-15% and 200-400 ml in adults or >12% in children after inhaling salbutamol.53 PEF reversibility and confirmatory tests must be completed before starting asthma treatment. Immune responses protect the body from harmful bacteria, but allergens can trigger an overreaction, causing allergies. Symptoms include sneezing, coughing, wheezing, chest tightness, and shortness of breath. The same allergens causing asthma also stimulate Th-2 cells, which release cytokines like interleukin-4, 5, 13, and interferon-gamma, leading to lung inflammation and IgE secretion. Th17 cells, which secrete interleukin-6, 17, and 22, mediate neutrophilic inflammation. Dexamethasone treatment does not affect Th17 cytokine production but induces glucocorticoid receptor movement to the nucleus. Both Th2 and Th17 cells can induce airway hyperresponsiveness, but Th17-mediated inflammation is steroid-resistant. IL-4 is essential for initiating allergic airway and humoral reactions by regulating Th2 cell survival, proliferation, and IgE formation.54 The IL-4 receptor (IL4R) on chromosome 16p is key in Th2 cell development and IgE generation. Studies in IL4 mutant mice showed that IL-4 and its receptor are crucial for specific IgE induction and bronchial hyperresponsiveness. IL-13, located on chromosome 5q, maintains high baseline IgE levels and plays a role independently of IL-4. The IL4R and IL13R subunits mediate the actions of IL-4 and IL-13.55 Altered receptor expression and cytokine levels may influence the development of atopy and asthma.
Expected Results
Strategies for prevention of asthma
Hyperresponsiveness and Maternal diet
Identifying the causes of asthma is essential for prevention, but it is challenging due to factors that may be mistaken for causal ones. Interventions targeting asthma prevention are unlikely to succeed without identifying those at higher risk. Low-risk patients could suffer negative effects from such therapies. While genetic and epigenetic factors contribute to asthma risk, they can’t be altered yet, although future methods may exist. Currently, environmental control and allergen immunotherapy are commonly used preventative measures. This study focuses on immunologic therapies for primary prevention, though many interventions indirectly affect the immune response, making it hard to differentiate from non-immunologic treatments.56
Asthma susceptibility in fetuses is influenced by inherited and non-inherited factors, with 56 genes linked to juvenile asthma and 19 to adult asthma.57 These genes affect protein production, including cytokine and chemokine receptors, leading to growth and functional anomalies in various tissues. While genetic inheritance increases asthma risk, current gene discoveries only partially explain asthma heredity. Epigenetic factors also play a role. Although prenatal genetic screening may identify at-risk embryos, no interventions currently exist to alter gene inheritance; though modifying gene expression could be a potential future target for intervention.58
Microbiome and early pet exposure
The microbiome during pregnancy and after birth may influence asthma and atopic diseases. Indoor microbiomes, possibly influenced by pets, might also play a role.59 Exposure to microbes, such as in farm environments, has been linked to a reduced risk of asthma, supporting the hygiene hypothesis. This theory suggests that exposure to diverse microbes can lower asthma risk, as seen in studies showing lower asthma rates in children raised on farms. For example, Amish children, exposed to higher endotoxin levels, had significantly lower asthma rates than Hutt rite children.60 Early pet exposure, particularly to dogs, reduces the risk of sensitization to allergens. Children with two or more dogs in the home were reduced to develop hypersensitivity to cats or dogs. However, this exposure did not lower the risk of developing asthma or methacholine hyperresponsiveness. A study investigated that those exposed to pets in the first year had lower IgE levels, though atopy prevalence remained similar. Further research suggests pet ownership may alter the home microbiome, providing a farm-like environment that reduces hypersensitivity. The infant physiological study found that infants exposed to pets had a microbiome associated with a lower asthma risk.61 These findings illuminate the shielded symptoms of wide range of surrounding exposures, even for families without access to farms or pets.62
Medications and Probiotics
The avoidance of premature Asthma in children study found that inhaled corticosteroids (ICS) improved episode-free days, effects, and worsen in preschoolers at high risk for asthma.63 However, ICS did not avoid the onset of asthma or long-term lung working issues. Similarly, early treatment with antihistamines like cetirizine did not prevent asthma development, though some atopic subgroups may benefit.64 Also giving beneficial bacteria like Lactobacillus rhamnosus (LGG) to mothers or infants during pregnancy or after birth can reduce the chances of eczema. However, while some research showed benefits, others did not find elimination of eczema in babies. Despite a new, moderately small, controlled trial demonstrating a tendency to a reduced case of asthma at 5 years, the danger ratio was not statistically correct.65
Environmental control through allergen immunotherapy
Sensitization and allergen exposure increase the risk of asthma symptoms once asthma develops. Early exposure to shedding skin cells, dust mites, and fungi has been linked to asthma and later sensitization. Dampness, mould, and musty odours in homes alter the indoor microbiome and are link with a greater chance of lung infection. Reducing exposure to dampness and fungi may lower asthma morbidity in sensitive individuals.65 Dust mite sensitivity in early childhood predicts asthma onset, and reducing exposure can lessen asthma symptoms. The Canadian Asthma Primary Prevention Study found that avoiding allergens like tobacco smoke, pet dander, and dust mites reduced asthma development in high-risk infants, though no significant effect on atopy was observed after 2 years. The Prevent Allergy Treatment (PAT) research examined the impact of three years of hypodermic biotherapy on kids with allergic coryza and sensitivities to grass or birch pollen.66
Natural Antioxidants and Asthma
Curcuma longa: The WHO recognizes herbal medicines as essential for primary healthcare in developing countries like India, with 11-40% of asthma patients using them.66 Turmeric, particularly curcumin from Curcuma longa, has gained attention for its wide range of benefits, including anti-carcinogenic, anti-inflammatory, anti-diabetic and anti-oxidant properties. Curcumin modulates inflammation by inhibiting key signaling pathways like NF-kB, lowering the manufacturing of pro-inflammatory cytokines and proteins.67 Curcumin capsules help reduce airway obstruction, shown by improved FEV1 values in bronchial asthma patients.68 While clinical efficacy was limited, there was significant improvement in hematological parameters with minor symptoms, indicating that curcumin is a safe and effective supplementary treatment for asthma.69 A study found that Curcuma longa protected against lung inflammation, redox imbalance, and immune markers in hypersensitive animals. Its anti-allergic and redox imbalance effects were equal to or stronger than decadron, and its immunomodulatory activity improved Th1/Th2 balance. These findings highlighted Curcuma longa may be effective in treating asthma.66
Amla, or Indian gooseberry, is popular for its high ascorbic acid and antioxidant properties, which help in treating bronchial asthma. It strengthens the immune system, reduces inflammation, and supports respiratory health. Regular consumption of amla, either in juice or powder form, can help reduce asthma effects by increasing working of lungs, improving airflow, and reducing the frequency of asthma attacks. It may also help in lowering redox imbalance and inflammation in the airways, offering relief from respiratory conditions. Amla contains flavonoids like quercetin and kaempferol, which have anti-inflammatory and antioxidant effects.70 These compounds help reduce inflammation in the respiratory tract, improving breathing and lung function. Amla is rich in tannins, which has shown to have anti-inflammatory and antimicrobial activities, aiding in the reduction of inflammation and protection against respiratory infections. Popular for its redox imbalance and anti-inflammatory applications, gallic acid helps in reducing airway inflammation and controlling asthma symptoms. Ellagic acid has been found to have anti-inflammatory applications, which may contribute to reducing airway constriction in asthma.71
Ghee quath (or ghee kwath) is a traditional Ayurvedic remedy that combines clarified butter (ghee) with medicinal herbs, and is used in treating respiratory conditions such as bronchial asthma. While there is very few direct modern investigation precisely on “ghee quath” itself, the components used in its preparation—ghee and specific herbs—have been studied for their beneficial effects on asthma and respiratory health. Ghee is considered an effective substance to soothe dry, irritated airways by providing lubrication to the respiratory tract. This may help in reducing asthma symptoms like coughing and wheezing caused by dry or inflamed airways.72 The combination of ghee with herbs like turmeric and black pepper in ghee quath is known to provide potent anti-inflammatory effects. Turmeric contains curcumin, which has been widely studied for its ability to reduce airway inflammation in asthma patients. Ghee itself has also been found to support the reduction of inflammation, although more research is needed in the context of asthma specifically. Ayurvedic formulations containing ghee and herbs like ginger, long pepper, and turmeric are known to increase working of lungs and decrease the rate of asthma attacks by helping to open up the airways and reduce the bronchoconstriction typical in asthma. Ghee contains butyrate, a small fatty acid with anti-inflammatory and redox imbalance effects that may shield against oxidative stress in the lungs, a key factor in asthma. Ghee is considered a rasayana (rejuvenative) in Ayurveda, which means it can help strengthen the immune system and modulate immune responses. This could be beneficial for asthma patients, whose immune systems often overreact to allergens or irritants.72
Tulsi, or holy basil, is a fragrant herb native to India with a long past in Ayurvedic medicine. Known as the “Elixir of Life,” it treats various health issues like pyrexia, rheumatism, bronchitis, asthma, and inflammation. A study revealed that 500 mg of withered tulsi leaves eating thrice daily enhanced lung function and relieved asthma symptoms in just three days. Tulsi is a key ingredient in Ayurvedic cough syrups and expectorants, helping to clear mucus in bronchitis and asthma.73 Tulsi contains substances like eugenol and flavonoids that possess anti-inflammatory applications. These substances help decrease airway inflammation, a key feature in asthma. By modulating the inflammatory response, tulsi may reduce bronchial constriction and ease breathing difficulties. Tulsi has been found to exhibit bronchodilator effects, which help relax the muscles of the airways and improve airflow. This is particularly beneficial for asthma patients who experience bronchospasms and airway constriction. The antioxidant compounds in tulsi, such as flavonoids and polyphenols, help to decrease redox imbalance in the lungs. This is important because oxidative stress can trigger inflammation and exacerbate asthma symptoms. Tulsi also has immunomodulatory effects, meaning it help regulate the immune system.74 In asthma, the immune system often overreacts to allergens, and tulsi may help normalize immune responses, reducing allergic reactions and inflammation. Tulsi’s antimicrobial properties help protect against respiratory infections, which can worsen asthma symptoms. Its ability to fight infections may be beneficial for asthma patients prone to respiratory illnesses. A clinical study showed that tulsi leaves, when consumed in a standardized form (500 mg thrice a day), significantly improved lung function in asthmatic patients, reducing wheezing and shortness of breath The study also reported improved exhalation capacity in asthma patients after using tulsi.75
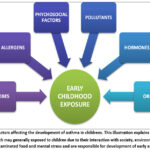 |
Figure 1: Factors affecting the development of asthma in childrens. This illustration explains the several factors which may generally exposed to children due to their interaction with society, environment, drugs, contaminated food and mental stress and are responsible for development of early asthma. |
 |
Figure 2: Phenotypic effects of asthma in pediatric patients. They are different observable patterns of the disease that vary among children due to factors such as genetics, environmental exposure, immune response, and age. Some children show airway inflammation and hyperresponsiveness, while others may exhibit poor response to traditional treatments. |
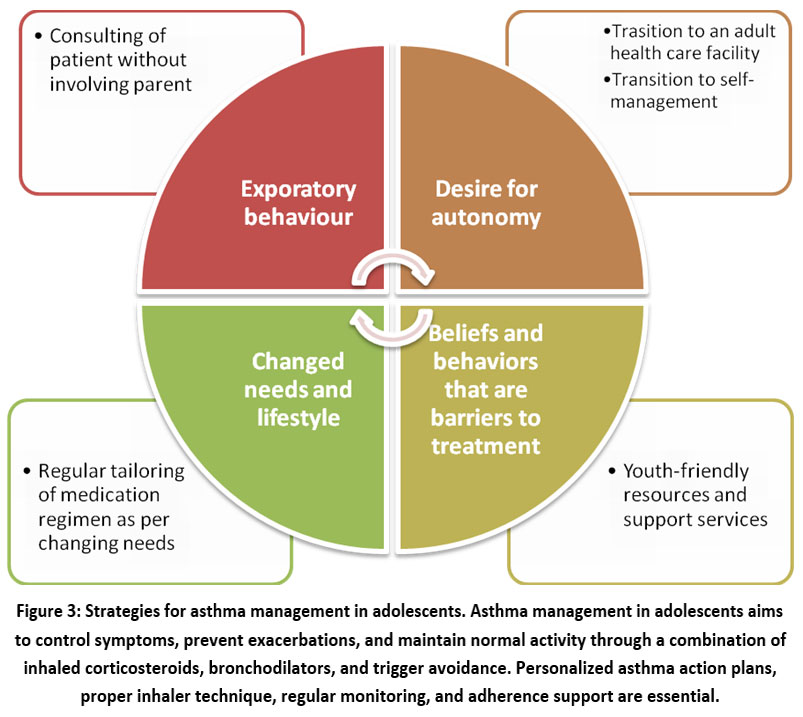 |
Figure 3: Strategies for asthma management in adolescents. Asthma management in adolescents aims to control symptoms, prevent exacerbations, and maintain normal activity through a combination of inhaled corticosteroids, bronchodilators, and trigger avoidance. Personalized asthma action plans, proper inhaler technique, regular monitoring, and adherence support are essential. |
Conclusion
The article on asthma in pediatric patients explores its pathophysiology, epidemiology, and underlying mechanisms to provide insights into better diagnosis, prevention, and treatment. It begins by detailing the biological processes, including airway inflammation, bronchoconstriction, and the use of white blood cells in the development of asthma. Epidemiologically, it highlights the generality of asthma in kids, risk factors, and environmental triggers, such as allergens and pollution. The article also discusses current diagnostic methods, including clinical assessments and testing, and emphasizes the importance of early diagnosis for effective management. Prevention strategies are outlined, focusing on reducing exposure to triggers and promoting healthy environments. Treatment approaches include pharmacological options (like bronchodilators and corticosteroids) and non-pharmacological strategies, such as allergen immunotherapy and lifestyle changes, aimed at improving quality of life and reducing exacerbations. It may be the pathophysiology, epidemiology, and mechanisms of asthma in pediatric patients are crucial for improving both diagnosis and management of the condition. Early identification, alongside a comprehensive approach to prevention and treatment, can significantly enhance outcomes for children with asthma. Advances in pharmacological treatments, environmental control strategies, and bespoke care are crucial to effectively managing asthma and reducing its effect on children’s quality of life. Continued research into the underlying mechanisms of asthma and the development of innovative therapies will be vital in further improving care and minimizing long-term complications for pediatric patients.
Acknowledgement
I would like to show our deep appreciation to the authors whose work has been referenced in this review. I also wish to thank Ankit Agrawal of School of Biotechnology, IFTM University and Basudev Banerjee of Department of Biochemistry, Santosh Deemed to be University whose data, studies, and insights have provided valuable context and support to this review article. Special thanks go to Tanzeel Ahmed for their encouragement and constructive feedback throughout the writing process. Without their dedication and collaboration, this article would not have been possible.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The author(s) do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
References
- Westerhof, G. A.; Coumou, H.; de-Nijs, S. B.; Weersink, E. J.; Bel, E. H. J. of. Aller. And. Clin. Imnlgy. 2018, 141(1), 104-109.
CrossRef - Moriarty, F. J. of. Mol. Med. 2020, 32(4), 1027-1033.
- McCauley, K. E.; Flynn, K.; Calatroni, A. J. Allergy. Clin. Immunol. 2022, 150, 204–13.
CrossRef - GBD Compare. Viz. Hub. 2021. https://vizhub.healthdata.org/gbd-compare
- Chung, K. F.; McGarvey, L.; Song, W. J.; Chang, A. B.; Lai, K.; Canning, B. J.; Birring, S. S.; Smith, J. A.; Mazzone, S. B. Nat. Rev. Dis. Primers. 2022, 8(1), 45.
CrossRef - Drake, M. G.; Cook, M.; Fryer, A. D.; Jacoby, D. B.; Scott, G. D. Front. Physiol. 2021, 12, 720538.
CrossRef - Brusselle, G. G.; Koppelman, G. H. N. Engl. J. Med. 2022, 386, 157–171.
CrossRef - He, L.; Zhou, X.; Mo, H.; Li, X.; Guo, S. Annals. Of. Palliative. Medicine. 2022, 11(2), 57487-57587.
CrossRef - Wang, P.; Zhao, W.; Sun, J.; Tao, T.; Zhu, M. S. J. Allergy. Clin. Immunol. 2018, 141(4), 1259-1268.e11.
CrossRef - Li, Z.; Chen, X.; Liu, Z.; Ye, W.; Li, L.; Qian, L.; Ding, H.; Li, P.; Aung, L. H. H. Front .Mol. Biosci. 2020, 7, 184.
CrossRef - Hamida, H.; Bart, N. Cell. 2021, 184(6), 1469-1485.
CrossRef - Miliku, K.; Azad, M. B. Nutrients. 2018, 10(8), 995.
CrossRef - Chapman , D. G.; Irvin, C. G. Clin. Exp. Allergy. 2015, 45(4), 706-19.
CrossRef - Hynes, G. M.; Hinks, T. S. C. E. R. J. Open. Res. 2020, 6.
CrossRef - Bazan-Socha, S.; Buregwa-Czuma, S.; Jakiela, B.; Zareba, L.; Zawlik, I.; Myszka. A.; Soja, J.; Okon, K.; Zarychta, J.; Kozlik, P. Int. J. Mol. Sci. 2021, 22, 998.
CrossRef - Burgoyne, R. A.; Fisher, A. J.; Borthwick, L. A. Cells. 2021, 10, 2763.
CrossRef - Mazari, A. M. A.; Zhang, L.; Ye, Z. W.; Zhang, J.; Tew, K. D.; Townsend, D. M. Biomolecules. 2023, 13(4), 688.
CrossRef - Kates, A. E.; Jarrett, O.; Skarlupka, J. H.; Sethi, A.; Duster, M.; Watson, L.; Suen, G.; Poulsen, K.; Safdar, N. Front. Cell. Infect. Microbiol. 2020, 10, 73.
CrossRef - Vercelli, D.; Bleecker, E. R. J. Allergy. Clin. Immunol. 2019, 144, 413-5.
CrossRef - Peterka, M.; Heringova, L. H.; Sukop, A. In. Vivo. 2021, 35(3), 1451–1460
CrossRef - Khalfaoui, L.; Pabelick, C. M. Expert. Opin. Ther. Targets. 2023, 27(1), 19-29.
CrossRef - Branco, A. C. C. C.; Yoshikawa, F. S. Y.; Pietrobon, A. J.; Sato, M. N. Mediators. Inflamm. 2018, 27, 9524075.
CrossRef - World Health Organization. Asthma. Report. 2021.
- Stein, M. M.; Hrusch, C. L.; Gozdz, J.; Igartua, C.; Pivniouk, V.; Murray, S. E. N. Engl. J. Med. 2016, 375(5), 411–21.
CrossRef - Lee-Sarwar, K.; Litonjua, A. A. J. Allergy. Clin. Immunol. Pract. 2018, 6(3), 711-718.
CrossRef - Mattiuzzi, C.; Lippi, G. Int. Arch. Allergy. Immunol. 2020, 181, 292-5.
- Ponce, M. C.; Sankari, A.; Sharma, S. StatPearls. Publishing. 2025.
CrossRef - Li, H. F.; Yan, L. P.; Wang, K.; Li, X. T.; Liu, H. X.; Tan, W. Respir. Res. 2019, 20(1), 38.
CrossRef - Chan, L.; Lin, W.; Mengju, L.; Ying, J.; Faming, W. Bldng. And. Env. 2024, 266, 112082.
CrossRef - Balić, A.; Vlašić, D.; Žužul, K.; Marinović, B.; Bukvić-Mokos, Z. Int. J. Mol. Sci. 2020, 21(3),741.
CrossRef - Kabesch, M.; Tost, J. Semin. Immunopathol. 2020, 42(1), 43-60.
CrossRef - Lee, J. U.; Kim, J. D.; Park, C. S. Yonsei. Med. J. 2015, 56(4), 877-86.
CrossRef - Laidlaw, T. M.; Mullol, J.; Woessner, K. M.; Amin, N.; Mannent, L. P. J. Allergy. Clin. Immunol. Pract. 2021, 9(3), 1133-1141.
CrossRef - Mikhail, I.; Grayson, M. H. Ann. Allergy. Asthma. Immunol. 2019, 123(4), 352-358.
CrossRef - Zhu, T.; Chen, Z.; Chen, G. Mediators. Inflamm. 2019, 24, 56-64.
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou E. Front. Public. Health. 2020, 8, 14.
CrossRef - Satpute, R. S.; Agrawal, A. A. Int. J. of. Int. Sys. And. App. In. Eng. 2023, 11(3s), 249–259.
- Liao, G.; Wang, R.; Tang, D. D. Am. J. Respir. Cell. Mol. Biol. 2022, 66, 223–234.
CrossRef - Meghji, J.; Mortimer, K.; Agusti, A. Lancet. 2021, 397, 928-940.
CrossRef - Loerz, C.; Maser, E. J. Steroid. Biochem. Mol. Biol. 2017, 174, 65-71.
CrossRef - Kistemaker, L. E. M.; Prakash, Y. S. Physiology. (Bethesda). 2019, 34(4), 283-298.
CrossRef - Chao, K. L.; Kulakova, L.; Herzberg, O. Proc. Natl. Acad. Sci. U S A. 2017, 14(7), 1128-1137.
- Lewis, B. W.; Ford, M. L.; Rogers, L. K.; Britt, R. D. Antioxidants. (Basel). 2021, 10(9), 1335.
CrossRef - Bae, D. J.; Jun, J. A.; Chang, H. S.; Park, J. S.; Park, C. S. Tuberc. Respir. Dis. 2020, 83, 1–13.
CrossRef - Lapin, B.; Piorkowski, J.; Ownby, D.; Freels, S.; Chavez, N.; Hernandez, E.; Wagner-Cassanova, C.; Pelzel, D.; Vergara, C.; Persky, V. Ann . Allergy. Asthma. Immunol. 2015, 114(3), 203-7.
CrossRef - Chowdhury, N. U.; Guntur, V. P.; Newcomb, D. C.; Wechsler, M. E. Eur. Respir. Rev. 2021, 30(162), 210067.
CrossRef - Dharmage, S. C.; Perret, J. L.; Custovic, A. Front. Pediatr. 2019, 7, 246.
CrossRef - Eguiluz-Gracia, I.; Mathioudakis, A. G.; Bartel, S.; Vijverberg, S. J.; Fuertes, E.; Comberiati, P.; Cai, Y. S.; Tomazic, P. V.; Diamant, Z.; Vestbo, J.; Galan, C.; Hofmann, B. Allergy. 2020, 75(9), 2170–2184.
CrossRef - Jeffrey, R.; Stokes, M. D.; Bacharier, M. D. Allergy. 2020, 125(2), 156-162.
CrossRef - Bellou, V.; Gogali, A.; Kostikas, K. J. Pers. Med. 2022, 12(8), 1231.
CrossRef - Sim, Y. S.; Lee, J. H.; Lee, W. Y.; Suh, D. I.; Oh, Y. M.; Yoon, J. S.; Lee, J. H.; Cho, J. H.; Kwon, C. S.; Chang, J. H. Tuberc. Respir. Dis. (Seoul). 2017, 80(2), 105-112.
CrossRef - Pinot-de-Moira, A.; Strandberg-Larsen, S.; Bishop, T. Journal. of. Allergy. And. Clinical. Immunology. 2022, 150(1), 82-92.
CrossRef - Sethi, L.; Bhadra, P. J. of. Nat. Sci. 2020, 10(60), 20854-20860.
- Gour, N.; Wills-Karp, M. Cytokine. 2015, 75(1), 68-78.
CrossRef - O’Byrne, P.; FitzGerald, J. M.; Bateman, E. D.; Barnes, P. J.; Zheng, J.; Gustafson, P. Lancet. Respir. Med. 2021, 9, 149–158.
CrossRef - Brunwasser, S. M.; Hartert, T. V. Clin. Chest. Med. 2019, 40, 1-11.
CrossRef - Johansson, E. K.; Bergström, A.; Kull, I.; Melén, E.; Jonsson, M.; Lundin, S.; Wahlgren, C. F.; Ballardini, N. J. Eur. Acad. Dermatol. Venereol. 2022, 36(5), 698-704.
CrossRef - Global Initiative for Asthma. A GINA pocket guide for health professionals. Version 3. Fontana. WI: Global. Initiative. For. Asthma. 2021.
- Karen, P. B.; Michael, G.; Declan, K.; James, M.; Maria, M. The. American. Journal. of. Clinical. Nutrition. 2016, 103(1), 128-143.
CrossRef - Sompornrattanaphan, M.; Thongngarm, T.; Ratanawatkul, P.; Wongsa, C.; Swigris, J. J. Asian. Pac. J. Allergy. Immunol. 2020, 38(1), 19–28.
- Pietruczuk, M.; Kraszula, L.; Kupczyk, M.; Kuna, P.; Eusebio, M. J. Biol. Regul. Homeost. Agents. 2021, 35(2), 485–94.
CrossRef - Ushio-Fukai, M.; Ash, D.; Nagarkoti, S.; Belin-de-Chantemèle, E. J.; Fulton, D. J. R.; Fukai, T. Antioxid. Redox. Signal. 2021, 34(16), 1319-1354.
CrossRef - Jackson, D.; Bacharier, L.; Gergen, P. J. Allergy. Clin. Immunol. 2022, 149, 146.
CrossRef - Cabana, M. D.; McKean, M.; Caughey, A. B.; Fong, L.; Lynch, S.; Wong, A. Pediatrics. 2017, 140, e20163000.
CrossRef - Mortimer, K.; Lesosky, M.; Garcia-Marcos, L. Eur. Respair. J. 2022, 60, 2200298.
CrossRef - Zhang, S.; Fan, Y.; Qin, L.; Fang, X.; Zhang, C.; Yue, J. Respir. Res. 2021, 22(1), 216.
CrossRef - Wang, R.; Wang, Y.; Liao, G.; Chen, B.; Panettieri, R. A.; Penn, R. B.; Tang, D. D. iScience. 2022, 25, 103833.
CrossRef - Ohara, Y.; Ohara, T.; Hashimoto, K.; Hosoya, M. Fukushima. J. Med. Sci. 2020, 66(2), 78–87.
CrossRef - Boskabady, M. H.; Amin, F.; Shakeri, F. Evidence-Based. Complementary. Altern. Med. 2021, 21, 257-264.
CrossRef - Scheer, F. A. J. L.; Hilton, M. F.; Evoniuk, H. L.; Shiels, S. A.; Malhotra, A.; Sugarbaker, R.; Ayers, R. T.; Israel, E.; Massaro, A. F.; Shea, S. A. Proc. Natl. Acad. Sci. U. S. A. 2021, 118(37), e2018486118.
CrossRef - Sathya, M. J. of. Ayu. And. Int. Med. 2015, 6(3), 186-192.
- Rodrigo-Munoz, J. M.; Gil-Martinez, M.; Lorente-Sorolla, C.; Garcia-Latorre, R.; Valverde-Monge, M.; Quirce, S.; Sastre, J.; Del-Pozo, V. Front. Immunol. 2022, 13, 858722.
CrossRef - Montgomery, M. T.; Sajuthi, S. P.; Cho, S. H. Am. J. Respir. Cell. Mol. Biol. 2020, 63, 172–84.
CrossRef - Behrooz, L.; Balekian, D. S.; Faridi, M. K.; Espinola, J. A.; Townley, L. P.; Camargo, C. A. Respir. Med. 2018, 140, 21-26.
CrossRef - Asher, M. I.; Rutter, C. E.; Bissell, K.; Chiang, C. Y.; El-Sony, A.; Ellwood, E. Lancet. 2021, 398, 1569-80.
CrossRef







ISSN Online: 2231-5039

![]()




{kind=link}